Let me start with a radical statement: I love data. One of my favorite activities in my role as chief strategy officer at Children & Families First, a large nonprofit child and family services agency, is turning columns of numbers into sets of colorful graphs. But even more satisfying is watching someone engage with the data as it reveals previously hidden meaning.
Let me start with a radical statement: I love data. One of my favorite activities in my role as chief strategy officer at Children & Families First, a large nonprofit child and family services agency, is turning columns of numbers into sets of colorful graphs. But even more satisfying is watching someone engage with the data as it reveals previously hidden meaning.
Since 2014, Children & Families First has been collecting Adverse Childhood Experience (ACE) data from the people we serve — both adolescents and adults. When we embarked on this journey, it was instinctual — some of our leadership had been introduced to the science of adversity, so we knew ACEs were important, and we wanted to understand how they impacted the people we serve — but we didn’t really have a plan for how to collect the data or what to do with it once we did. We simply armed our staff with a stack of questionnaires and sent them out into the field to ask their clients 10 incredibly difficult questions. Amazingly, they asked and our clients answered.
Over time, as we collected more and more surveys, it became clear to us that we needed two things:
- a clear set of guidelines for staff to use to collect the data so that the process was both consistent and trauma-informed, and
- a way to pair resilience concepts with the ACEs survey so that our clients could understand that despite their experiences of adversity, resiliency can be built throughout a lifetime.
We convened a group of staff who were interested in the work — our ACE Protocol Task Force — and set about developing protocols and guidance and to identify resiliency tools. We borrowed heavily from the great work that was being done by others across the nation — like the National Crittenton Foundation, Thrive Washington and the Center for Youth Wellness to name a few. We selected the Devereux Adult Resiliency Survey as our resiliency tool and made a simple modification for use with adolescents. (We selected this tool for both its ease of use and its positive, future-focused language.)
In developing the protocol, we had many conversations with our program staff about what the ACEs collection process should look like in each of their units: Would we have folks complete the ACE questionnaire directly so that we had data about specific ACEs or would we simply ask our clients to review the questionnaire and tell us their score? In some instances, could we mine the record to get a sufficient ACE snapshot? Would we use the Devereux Resiliency Survey as a benchmark or a pre- and post-assessment to determine if our intervention had any resilience-building effects?
In the end, we settled on a blended approach, with each unit determining the best fit for their service-delivery and client needs. We then set about training every unit in both the underlying brain science concepts (a refresher for most) and the protocol itself.
As the completed questionnaires began to roll in, I had the privilege of tabulating responses and turning the data into pictures. And what the data revealed was somehow both unsurprising and shocking at the same time: The kids and families we serve have experienced trauma at rates much higher than that found in the original ACE study. Our children and families are almost three times as likely to have experienced four or more ACEs as those in the original study population (37 percent as compared to 13 percent).
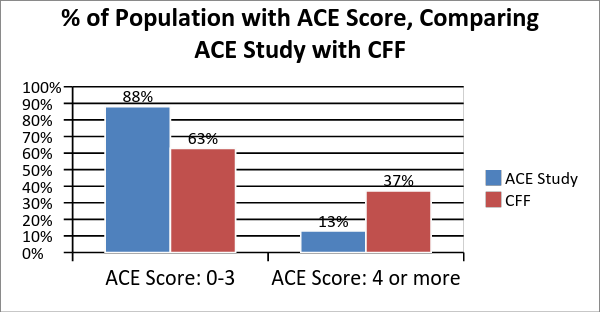
ACE Study data found here
Among certain program populations, the results are even more striking. Nearly three-quarters of the youth in our foster care program have experienced four or more ACEs and almost 10 percent have experienced all 10. When I sent the manager of our foster care program the charts and graphs I had compiled, she was taken aback, telling me in hushed tones, “I knew our kids had experienced trauma, but seeing it like this is really eye-opening.”
But that’s only one side of the story. As guided by our ACE Data Collection Protocol, we have also begun to gather resilience data from our clients, and the early results are promising. More than 75 percent of clients surveyed at enrollment in services indicate that they already have “resiliency in place.” They show the strongest resilience around their internal beliefs in themselves — affirming statements like: I have personal strengths; I have strong beliefs; and I am hopeful about the future. This tells us that in spite of adversity, or perhaps even because of it, our clients are finding ways to build beliefs, skills and supports to help them achieve well-being.
This experience has been incredibly valuable for us as an organization, in a number of ways. First, it has helped elevate the conversation about ACEs to the forefront of our work, across programs and services. Concepts around adversity, toxic stress and resilience have become foundational to our work.
Second, for an agency that provides more than 20 different services to thousands of individuals each year, we have struggled to find common measures across our work. Each program not only provides different services, but also uses different assessment tools, sets different goals and priorities, and measures different outcomes.
ACEs and resilience have changed that — we now have a common set of data to help us understand and describe the people we serve across the organization, regardless of which door they come through. Finally, when we know more, we can do better. We understand that toxic stress has a significant impact on the brains and bodies of developing children, and we know that resilience can be built across a lifetime. This knowledge helps us deliver on our mission to help children and families facing adversity on their journey to adulthood, by supporting families to raise their children so they can flourish.
Kirsten Olson has worked in the nonprofit human services sector for more than 20 years, providing services and supports across a variety of target populations including the homeless, persons with behavioral health conditions and youth in child welfare. She is chief strategy officer at Children & Families First, where she is responsible for program evaluation and outcomes management for the agency’s more than 20 program areas.