Just 5 percent of youth with a substance use disorder get treatment
“Addiction is a pediatric disease,” according to John R. Knight, M.D., the founder and director of the Center for Adolescent Substance Abuse Research at Boston Children’s Hospital. “When adults entering addiction treatment are asked when they first began drinking or using drugs, the answer is almost always the same: They started when they were young — teenagers,” said Knight.
Smoking, drinking and some forms of drug use among teens have declined in the U.S. in recent years. But with more than 2 million adolescents currently reporting use of an illicit drug, the problems of teenage substance abuse are far from resolved.
Drug use changes brain development, and when substances are used during adolescence, young people are much more likely to become addicted, Knight
said.

Hurt. Grief. Guilt. Sisters, brothers reflect on dead siblings’ drug addictions.
“When people start using at younger ages, the changes in brain structure and function are very, very pronounced,” he explained.
“If we could only get kids to postpone their first drink or their first use of drugs, we could greatly diminish the prevalence of addiction in the U.S.,” he said.
More severe addictions
“In the last several years, it seems like the kids that we see in services are far sicker than in the past,” said Sara Ellsworth, clinical supervisor at True North Student Assistance and Treatment Services in Olympia, Wash. Last year, True North served nearly 700 students in 44 mostly rural school districts.
Despite some improvements in the national youth substance abuse numbers, Ellsworth has witnessed a disturbing new pattern: kids who start using alcohol or marijuana at ever younger ages, who quickly escalate to more dangerous drugs, and who wind up using multiple substances in extreme amounts. “Maybe the average kid is using less and doing better, but the kids who are falling through the cracks are spiraling down, really fast,” she said.
About 10 percent of the population will develop a substance-use disorder and need therapeutic services, according to Rob Vincent, a public health analyst at SAMHSA, the Substance Abuse and Mental Health Services Administration. But those services are hard to come by, especially for youth.
“Once a child 12 to 17 years old is identified as needing treatment, only one in 20 of those adolescents is actually getting treatment. That is not a good number,” said Vincent. He said dealing with drug and alcohol abuse after the fact is a costly, impractical approach, which has led experts to embrace early detection and intervention. “In the best of all worlds, we would prevent a substance use disorder from ever occurring,” Vincent said.
Screening: the first step
The leading prevention strategy, dubbed SBIRT — Screening, Brief Intervention and Referral to Treatment — is now deployed in schools, some after-school programs and, most widely, in primary care and public health.
Most pediatricians now routinely screen patients for substance problems during annual visits. That’s a big change from just 20 years ago when the American Academy of Pediatrics (AAP) found fewer than half (45 percent) of pediatricians reported they were screening adolescents for substance use. By 2013, that percentage had risen to more than 80 percent.
“I interpret that as a real shift in culture, from one in which there was controversy over whether drug use was a legitimate topic for pediatricians to address to one in which it’s now part of the standard of care,” said Sharon Levy, M.D., director of the Adolescent Substance Abuse Program at Boston Children’s Hospital.
Levy, who also teaches pediatrics at Harvard Medical School, sees the pediatrician’s office as an ideal place to talk about substance abuse. “It’s a unique setting in which an adolescent gets to have a confidential conversation one-on-one” with an adult who is not their parent.
In step one of the SBIRT approach, doctors use one of a variety of specially designed screening tools suited for an office visit. CRAFFT, one of the earlier tools recommended by the AAP, and developed by Dr. Knight, asks kids a series of six questions designed to detect problems related to alcohol or drug use. In many doctors’ offices, the survey is now computerized or given as a questionnaire before the medical visit, so the pediatrician can discuss the results.
Other screening tools widely in use are called frequency-based screens. Those tools use multiple-choice questions that ask kids how often they have used alcohol or marijuana within several specified timeframes to predict their risk of developing an addiction.
Brief intervention
The second step of SBIRT is brief intervention. In the doctor’s office, that could be a five-minute conversation with the two elements that Knight says comprise a good brief intervention: science and stories. “Youth tell us in focus groups and interviews that what they want from doctors is, ‘Tell us what the science is, don’t tell us what to do; give us the information, and trust us to make the right decisions.’”
Screeners can also be therapists, counselors or youth-development workers. They often use what’s called “motivational interviewing” in the intervention.
Elizabeth D’Amico, a licensed clinical psychologist and senior behavioral scientist at RAND Corporation, developed CHOICE, a voluntary after-school prevention/intervention program in California, using that approach. “Motivational interviewing is about guiding someone to make a healthy choice, versus saying, ‘Okay, you have a problem and you need to change.’”
According to D’Amico, counselors have to acknowledge there are reasons why young people use alcohol or drugs. “You lose all your credibility if you just say, ‘It’s bad for you, stop.’”
Instead, motivational interviewing is more collaborative, said D’Amico. For example, if a teen says he drinks to relax, the counselor can help him to think of other, healthier ways to relieve stress.
The third step of a prevention strategy — referral to treatment — tries to connect youth who need more extensive care with specialty treatment. Levy said the vast majority of kids with a drug or alcohol problem don’t need a residential rehab program, or even an intensive outpatient program. “Many of the kids who have substance use disorders might do fine to work one-on-one with a counselor,” she said.
School-based interventions
Along with pediatricians, schools are actively involved in prevention, starting as early as elementary school, when entire grades receive a universal prevention program. One popular curriculum, called the Good Behavior Game, is a classroom presentation. As part of the game, children learn how to resist peer pressure, while receiving the message that drugs aren’t good. According to one evaluation by researchers at Johns Hopkins University, children who had played the Good Behavior Game when they were young were less likely to smoke or to have a drug- or alcohol-use disorder 15 years later as young adults.
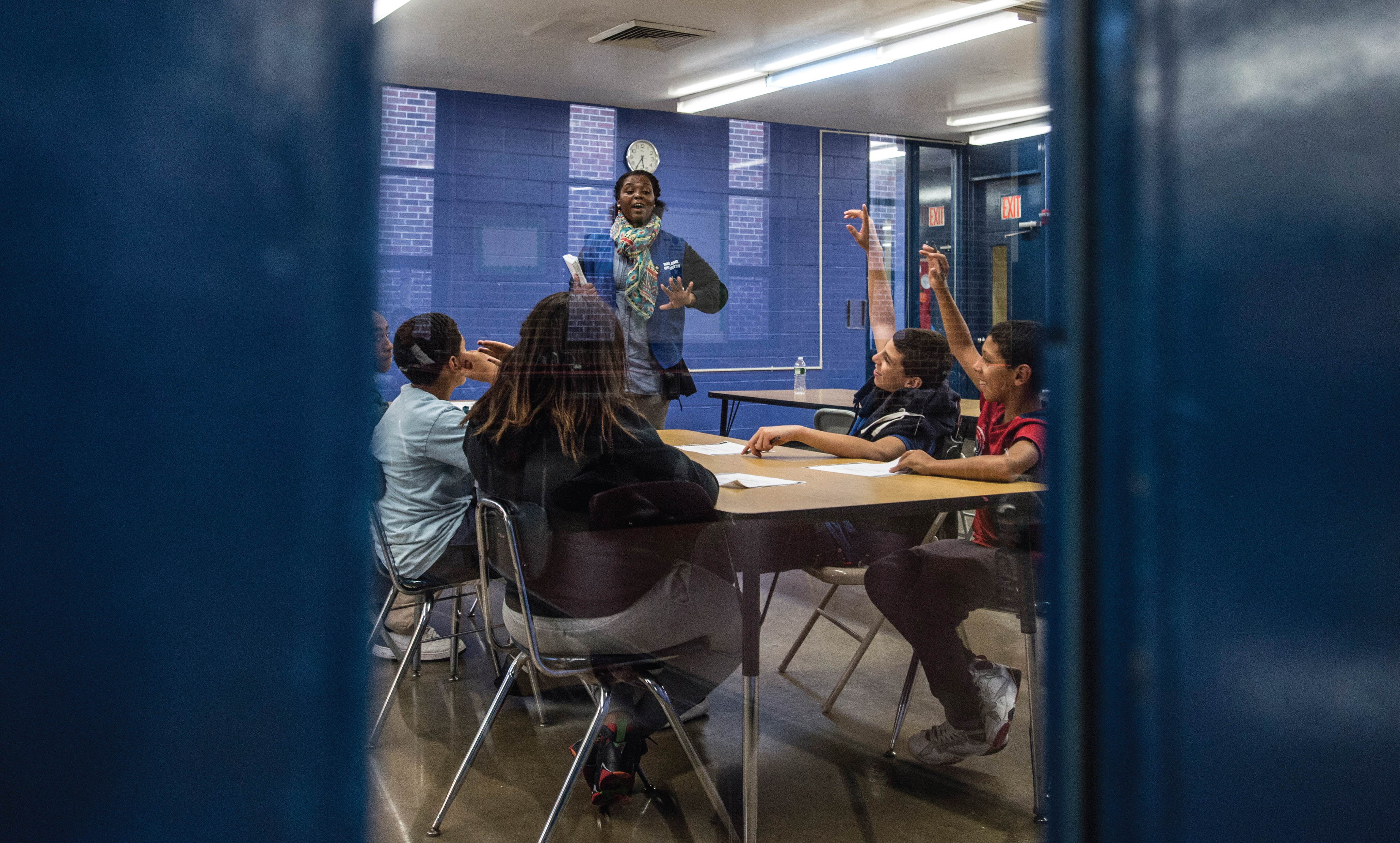
Two hundred teens each year participate in an evidence-based curriculum at Madison Square Boys & Girls Club in a program called Empowerment, funded by the New York State Office of Alcohol and Substance Abuse Services.
Targeted intervention comes later. By the time individual students at True North in Washington State are referred for treatment, they usually have shown high-risk factors for substance abuse or have been busted for a drug or alcohol infraction, said clinical supervisor Ellsworth. Because the program is school-based, students have easy access to services and the bonus of a powerful motivator. “If a student has a disciplinary referral for substance use, they face a 45-day suspension that can be reduced to five days if they agree to services,” said Ellsworth.
Treatment options include individual or group counseling, which can extend to ongoing support of a child who is trying to stay clean and sober. Ellsworth has watched students in recovery go from failing to a spot on the honor roll. She recalled one 15-year-old girl whose family had a history of drug abuse. She was caught smoking marijuana in sophomore year, had intensive outpatient treatment — and relapsed more than once — but eventually entered senior year with more than a year in recovery, good grades and a promising future.

Messaging about strength, courage and wisdom greets kids at Madison Square Boys & Girls Club, just one of many clubs nationwide bringing substance use prevention curricula to after-school programming.
More than 2,400 schools nationwide have joined the movement to provide comprehensive health services on site, establishing school-based health centers. More than half of these school-based clinics (53 percent) provide substance abuse counseling, and nearly 10 percent have a trained alcohol and drug counselor on staff, according to the School-Based Health Alliance.
But in many districts, non-academic programs are losing out to growing demands on the school day. Prevention programs and similar activities “are getting pushed out of class time because of the pressures on schools with standardized testing and other things,” said D’Amico. After-school programs have been trying to fill the vacuum.
Prevention after school
More than half (57 percent) of the nation’s Boys & Girls Clubs of America (BGCA) are involved in substance use prevention, using a program called SMART Moves, designed to help kids avoid tobacco, alcohol and drugs. Developed in the 1980s by prevention specialists and BGCA staff, SMART Moves offers three core programs for different age groups, as well as a peer leader program for teenagers and a family advocacy network to get parents involved.
The SMART (Skills Mastery and Resistance Training) programs, which were updated in 2011, focus on educating kids about the dangers of substance use and dispelling the myth that “everybody’s doing it.” The program works on developing kids’ protective factors, such as good decisionmaking, maintaining friendships and dealing with peer pressure.
Through interactive games and social scenarios, club members learn about the consequences of drug use while still having fun. Dawn McDaniel, a senior director of BGCA’s Gender & Wellbeing programs, said SMART “provides a real-world perspective with a lot of opportunity for youth to reflect about what’s going on their own communities.”
Some clubs use different programs to address substance prevention as a part of a healthy lifestyles curriculum. Regardless of curricula, BGCA capitalizes on the relationships staff often develop with club members to promote prevention. “We have club members who enter at age 6, and we’ll see them remain in the club until they’re 18. Those relationships are really important, so kids have somebody they go to when they have hard decisions to make,” said McDaniel.
Does prevention work?
Outcomes research from the SMART program in 1992 (the last formal evaluation) showed children who attended the program had better knowledge and refusal skills, along with lower rates of drug use than children who didn’t attend. McDaniel has been pushing for an updated evaluation to make sure that those positive outcomes have been maintained.
True North Student Assistance and Treatment Services also found that students served by the prevention programming had positive results. “What we see across the board is a reduction in use from the time they were screened to after services,” said Ellsworth. For the last academic year, the program saw marijuana and cocaine use decline by half, alcohol use decline by one-third, and amphetamine use decline by 43 percent. Students who participated in the program also had better grades and fewer behavior problems at school.
Even the computerized CRAFFT screening with two to three minutes of counseling by a pediatrician has been shown to deter substance use, according to a study led by Knight and published in the journal Pediatrics. “The intervention resulted in 40 percent less substance use three months after the visit, and 12 months later there was still 25 percent less use, without any reinforcement. That’s pretty powerful,” said Knight.
Prevention is also a cost-effective proposition, according to the National Institute on Drug Abuse (NIDA), with every dollar invested in keeping kids off drugs saving from $4 in health care costs to $7 in law enforcement and other criminal justice costs.
According to NIDA, research-based prevention programs can significantly reduce early use of tobacco, alcohol and illicit drugs. Yet according to Knight, “of all the money that is spent by the federal government on the so-called war on drugs, only 5 percent goes to prevention.” That’s a short-sighted approach, he said. “The evidence is compelling that addiction is a pediatric disease, and if we don’t prevent it during the teen years, we’re really missing the boat,” said Knight.
Prevention in the Club
Madison Square Boys & Girls Club, which operates four clubs in Brooklyn and the Bronx in New York, reaches about 200 14- to 18-year-olds with an evidence-based curriculum called Project Toward No Drug Abuse. The Club’s program, called Empowerment, is funded by the New York State Office of Alcohol and Substance  Abuse Services and addresses substance abuse prevention as a holistic healthy lifestyles curricula.
Abuse Services and addresses substance abuse prevention as a holistic healthy lifestyles curricula.
The program, engaging 12 to 15 teens in 10-week cycles, culminates in a community service project that teens implement in their neighborhoods, explained Thomas Bromage, director of program services.
Last year, 11 Empowerment members and two alumni created a mobile graffiti wall in support of National Drug Facts Week, showcasing art, statistics on drug abuse, myths about addiction and photos. This informative art piece was housed at Madison Square Boys & Girls Club’s Columbus Clubhouse and at a neighboring high school. “The members of Empowerment selected this project because teens in their community are introduced to drugs and alcohol more and more by their peers,” Bromage said in an email. “They believed that learning the facts about drugs would help their friends and peers make more informed, positive decisions.”
Substance abuse & teens: A long story
In the 1980s, drug and alcohol prevention moved into the national spotlight with first lady Nancy Reagan famously urging youth to “Just say no.” Within a decade, The Substance Abuse Prevention and Treatment Block Grant (SABG) was funding programs in all 50 states. With $1.8 billion in grants this year, SABG funds everything from TV spots encouraging parents to talk to their kids about drugs, to targeted screening and intervention for people who already have a problem. The grants flow from Washington, D.C., through state and municipal governments, often to community organizations that run prevention programs at the local level.
“You can’t treat your way out of this problem, and you can’t lock up enough people to solve the problem,” said Maj. Gen. Arthur T. Dean, (Ret.), currently the chairman of the Community Anti- Drug Coalitions of America (CADCA).
The nation’s Drug Free Communities Act created “our nation’s first line of defense when it comes to reducing youth drug use,” said Dean. Last year the program provided $93.5 million in the form of small grants of up to $125,000 per year for communities to tackle substance abuse in their neighborhoods. The nation’s 5,000 community anti-drug coalitions pull together sectors such as law enforcement, civic and business leaders, and parent and youth groups to build drug-free communities. CADCA comes to town and trains local residents to assess a community’s drug problems and then develop a strategic plan for change.
Dean cited a coalition in Rhode Island that discovered in 2009 that nearly one in five of their high school seniors was abusing prescription drugs. The coalition mobilized, setting up parent and youth training groups, launching a media campaign and funding an information project in the schools. Coalition members worked with police and pharmacists, and created a program for residents to turn in unused medication. Within five years, said Dean, the rate of prescription drug abuse had declined by roughly 60 percent.
Prevention strategies also have a substantial impact on school dropout rates, poor academic performance, truancy and other costly social problems. The payoff in reduced violence, motor vehicle crashes and gang-related crime has given rise to more than 400 juvenile drug courts in the U.S., where specially trained judges maintain close oversight of cases. For a year or more, a team of specialists from social and mental health services, schools and juvenile justice work with a young person and family members to address the substance use and related problems that got the young person into trouble.
Youth substance use at a glance
- An estimated 2.2 million adolescents — 8.8 percent of youth aged 12 to 17 years old — are currently using an illicit drug, according to a 2014 Behavioral Health Barometer prepared for the Substance Abuse and Mental Health Services Administration.
- Alcohol use among U.S. middle and high school students dropped last year to its lowest level since the 1970s, according to the University of Michigan’s “Monitoring the Future” study. This annual survey of up to 50,000 students found binge drinking fell significantly, and cigarette smoking reached historic lows, down to 8 percent of U.S. teens.
- Use of some illicit drugs, including hallucinogens like LSD, narcotics and some prescription drugs, was also down dramatically. The greatest decline was in students’ use of synthetic marijuana, known as K-2 or Spice.
- But not all the news is good: Roughly one in five high school seniors reported binge drinking (consuming five or more drinks in a row) in the prior two weeks, and one in four students surveyed reported smoking marijuana within the prior year.
- Use of some particularly dangerous drugs, such as amphetamines and cocaine, was unchanged. And while tobacco use has declined, e-cigarette consumption skyrocketed in the past year to include 17 percent of 12th graders.
CRAFFT
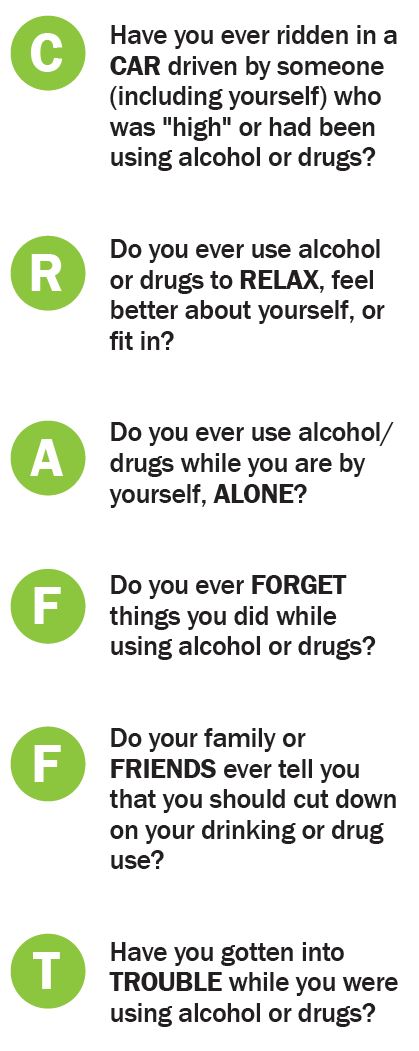 The CRAFFT, from www. ceasar-boston.org/CRAFFT/, is a behavioral health screening tool for use with children under the age of 21 and is recommended by the American Academy of Pediatrics’ Committee on Substance Abuse for use with adolescents. It consists of a series of six questions developed to screen adolescents for high risk of alcohol and other drug use disorders simultaneously. It is a short, effective screening tool meant to assess whether a longer conversation about the context of use, frequency, and other risks and consequences of alcohol and other drug use is warranted.
The CRAFFT, from www. ceasar-boston.org/CRAFFT/, is a behavioral health screening tool for use with children under the age of 21 and is recommended by the American Academy of Pediatrics’ Committee on Substance Abuse for use with adolescents. It consists of a series of six questions developed to screen adolescents for high risk of alcohol and other drug use disorders simultaneously. It is a short, effective screening tool meant to assess whether a longer conversation about the context of use, frequency, and other risks and consequences of alcohol and other drug use is warranted.
Screening using the CRAFFT begins by asking the adolescent to “Please answer these next questions honestly”; telling him/ her “Your answers will be kept confidential”; and then asking three opening questions.
If the adolescent answers “No” to all three opening questions, the provider only needs to ask the adolescent the first question — the CAR question. If the adolescent answers “Yes” to one or more of the three opening questions, the provider asks all six CRAFFT questions.
CRAFFT is a mnemonic acronym of first letters of key words in the six screening questions. The questions should be asked exactly as written.
Self-administered CRAFFT screening questions are available at ceasar-boston.org/CRAFFT/selfCRAFFT.php.
Resources
- Substance Abuse and Mental Health Services Administration (SAMHSA), www.samhsa.gov, is the federal agency that leads public health efforts to reduce the impact of substance abuse and mental illness on America’s communities.
- National Institute on Drug Abuse, www.drugabuse.org, part of the National Institutes for Health, has a long list of publications on the science of drug abuse and addiction, as well as information on prevention strategies for parents, educators and community leaders.
- Community Anti-Drug Coalitions of America, www.cadca.org, is a membership organization representing more than 5,000 coalitions working to make their communities safe, healthy and drug-free.
- Office of National Drug Control Policy, www.WhiteHouse.gov/ONDCP, a component of the executive branch, advises the president on drug-control issues, and coordinates national drug-control activities and strategies.
- Center for Adolescent Substance Abuse Research (CeASAR), www.ceasar-boston.org., at Boston Children’s Hospital is a leader in discoveries pertaining to prevention, diagnosis and treatment of substance-related disorders in children and adolescents.
- Teen-Safe, www.teen-safe.org, is a public service website developed by CeASAR, with materials about substance use for schools, parents and young people.